U.S. Department of Health and Human Services
NATIONAL INSTITUTES OF HEALTH NIH News
National Cancer Institute (NCI) <http://www.nci.nih.gov/>
Embargoed for Release: Monday, May 21, 2012, 11:05 a.m. EDT
CONTACT: NCI Press Office, (301) 496-6641, <e-mail: ncipressofficers@xxxxxxxxxxxx>
NIH STUDY FINDS SIGMOIDOSCOPY REDUCES COLORECTAL CANCER RATES
Flexible sigmoidoscopy, a screening test for colorectal cancer that is less invasive and has fewer side effects than colonoscopy, is effective in reducing the rates of new cases and deaths due to colorectal cancer, according to research sponsored by the National Cancer Institute, part of the National Institutes of Health. In a study that spanned almost 20 years, researchers found that overall colorectal cancer mortality (deaths) was reduced by 26 percent and incidence (new cases) was reduced by 21 percent as a result of screening with sigmoidoscopy. These results appeared online, ahead of print, on May 21, 2012, in the New England Journal of Medicine, and were presented at Digestive Disease Week <http://www.ddw.org/>, a scientific conference.
Sigmoidoscopy involves examination of the lower colon using a thin, flexible tube-like instrument, called a sigmoidoscope, to view the anus, rectum, and sigmoid colon (see Figure 1). Sigmoidoscopy has fewer side effects, requires less bowel preparation, and poses a lower risk of bowel perforation (an uncommon event, when the screening instrument pokes a hole in the intestine) than colonoscopy, in which a similarly flexible, but longer, tube is used to view the entire colon.
Colorectal cancer is the second-leading cause of cancer-related death in the United States. Previous research has shown that colorectal cancer incidence and mortality can be reduced with a number of screening methods, including fecal occult blood testing
<http://benchmarks.cancer.gov/2010/03/the-role-of-fecal-occult-blood-testing-in-colorectal-cancer-screening/> (FOBT). However, flexible sigmoidoscopy and colonoscopy are more sensitive than FOBT for detecting polyps (see Figure 2) that may lead to colorectal cancer. Removal of pre-cancerous polyps, which can be done during sigmoidoscopy or colonoscopy, reduces colorectal cancer risk.
"The most important message is that, regardless of modality chosen, colorectal cancer screening lowers mortality from colorectal cancer, and all individuals 50 and over should be screened," said study author Christine Berg, M.D., chief of NCI's Early Detection Research Group and project officer of the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial <http://dcp.cancer.gov/plco>.
>From 1993 to 2001, a total of 154,900 men and women aged 55 through 74 were randomly assigned to receive flexible sigmoidoscopy screening or usual care as part of the PLCO trial. People in the usual care group (i.e. control group) only received screening if they asked for it, or if their physician recommended it. This large population-based randomized trial was designed to determine the effects of screening on cancer-related mortality. Participants assigned to the flexible sigmoidoscopy group were screened once on entering the study (baseline) and again three years to five years later. The participants were followed for approximately 12 years to collect data on cancer diagnoses and deaths (additional background on PLCO) <http://dcp.cancer.gov/plco/background>.
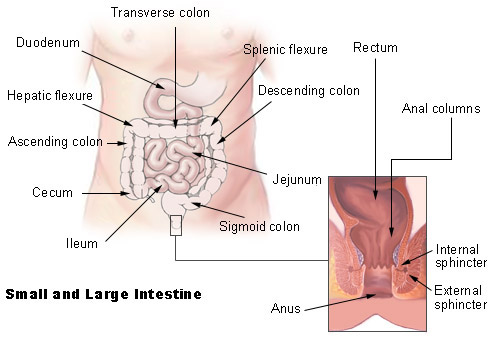
The researchers compared overall colorectal cancer mortality and incidence in the two groups, and also analyzed incidence and mortality according to the location of the cancers that developed. Cancers located from the rectum through a bend in the colon called the splenic flexure (see Figure 3) were defined as distal, and those in the transverse colon to the cecum were defined as proximal. Although flexible sigmoidoscopy examines only the rectum and sigmoid colon, participants with a suspicious finding were referred for a follow-up colonoscopy, in which both the distal and proximal regions of the colon would be examined.
Overall, after an average of nearly 12 years, participants in the screening group had a 21 percent lower incidence of colorectal cancer overall and a 26 percent lower rate of colorectal cancer mortality than participants in the usual care group. This means that, over the course of 10 years, if 1,000 people followed the PLCO protocol of two sigmoidoscopy screenings, there would be approximately three fewer new cases and one fewer death from colorectal cancer than in a comparable group not receiving regular screenings. The incidence of distal colorectal cancer was reduced by 29 percent, and mortality from distal colorectal cancer was reduced by 50 percent, in the screening group. While there was no statistically significant decline in deaths from proximal colorectal cancer, the incidence of proximal colorectal cancer was reduced by 14 percent in the screening group.
"This is the second major trial that has shown that sigmoidoscopy is effective in reducing the risk of dying of colorectal cancer. Sigmoidoscopy is less invasive than colonoscopy and carries a lower risk of the colon being perforated, which may make it more acceptable as a screening test to some patients," said Barnett Kramer, M.D., director of NCI's Division of Cancer Prevention. "There are several effective screening tests for colorectal cancer <http://www.cancer.gov/cancertopics/factsheet/detection/colorectal-screening>, and the most effective screening test is the one that people choose to take."
Screening by sigmoidoscopy detected 24 percent of the colorectal cancers that were diagnosed in the screening group. Another 60 percent were detected by symptoms or by screening performed outside of the PLCO protocol or were found more than one year after a screening exam -- the cutoff for defining a cancer as screen detected -- in participants who had at least one screening exam, and the remaining 16 percent developed in participants assigned to the screening group who never actually underwent screening. Of the colorectal cancers that were detected by screening, nearly 83 percent were found in the distal colon, whereas distal colorectal cancers made up about 53 percent of the cancers in people in the screening group who were never screened and about 32 percent of cancers in people who underwent screening but whose cancers were not detected by screening. Cancers detected by screening were more likely to be early stage (75 percent were stage I or II) than cancers that weren't detected by screening (51 percent were stage I or II). Screening was associated with reductions in incidence and mortality for all stages of distal colorectal cancer. However, in the proximal colon, reductions in incidence were only seen in stages I, II, and III, and there was no impact on proximal colorectal cancer mortality.
The researchers estimated that if they had used colonoscopy rather than sigmoidoscopy in this study, they would have identified 16 percent more cancers, two-thirds of which would have been proximal cancers. However, they were not able to determine what effect that may have had on proximal colorectal cancer mortality. There has been some controversy about how effective colonoscopy is in decreasing colorectal cancer mortality in different regions of the colon, with some studies suggesting that it is more effective against distal than proximal tumors. Sigmoidoscopy has never been directly compared to colonoscopy in a definitive clinical trial.
False-positive <http://www.cancer.gov/dictionary?cdrid=340929> sigmoidoscopy results were observed in 20 percent of men and 13 percent of women in the screening group, but some of these false positives could have been the result of false-negative colonoscopies done to follow up on suspicious sigmoidoscopy findings. Approximately 22 percent of people in the screening group were sent for follow-up colonoscopies during the screening phase of the trial.
The NCI's Division of Cancer Prevention <http://dcp.cancer.gov/> funded this research under contracts to the 10 PLCO screening centers and a coordinating center (N01-CN-25476, N01-CN-25511, N01-CN-25512, N01-CN-25513, N01-CN-25514, N01-CN-25515, N01-CN-25516, N01-CN-25518, N01-CN-25522, N01-CN-25524, and N01-CN-75022).
An overview of the PLCO trial results with perspectives in light of the end of the trial has just been published on our news blog at <http://benchmarks.cancer.gov/2012/05/overview-of-the-prostate-lung-colorectal-and-ovarian-plco-cancer-screening-trial>
A Q&A about the PLCO trial is available at <http://www.cancer.gov/newscenter/pressreleases/2012/PLCOQandA>
NCI leads the National Cancer Program and the NIH effort to dramatically reduce the burden of cancer and improve the lives of cancer patients and their families, through research into prevention and cancer biology, the development of new interventions, and the training and mentoring of new researchers. For more information about cancer, please visit the NCI website at <http://www.cancer.gov> or call NCI's Cancer Information Service at 1-800-4-CANCER (1-800-422-6237).
About the National Institutes of Health (NIH): NIH, the nation's medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit <www.nih.gov>.
NIH...Turning Discovery into Health
------------------------------------
REFERENCE: Shoen RE, Pinsky PF, Weissfeld L, Yokochi LA, Church T, Laiyemo AO, Bresalier R, Andriole GL, Buys SS, Crawford ED, Fouad MN, Isaacs C, Johnson CC, Reding DJ, O'Brien B, Carrick DM, Wright P, Riley TL, Purdue MP, Izmirlian G, Kramer BS, Miller AB, Gohagan JK, Prorock PC, and Berg CD. Colorectal Cancer Incidence and Mortality in the PLCO Screening Trial. NEJM. June 21, 2012.
------------------------------------
This release contains three images:
Figure 1: A thin, lighted tube is inserted through the anus and rectum and into the lower part of the colon to look for abnormal areas. Credit: Terese Winslow for NCI
<http://visualsonline.cancer.gov/retrieve.cfm?imageid=7182&dpi=72&fileformat=jpg>
Figure 2: Colon polyps are growths that can lead to colon cancer. They can be flat or have stalks as show. Credit: Terese Winslow for NCI
<http://visualsonline.cancer.gov/retrieve.cfm?imageid=7180&dpi=72&fileformat=jpg>
Figure 3: Segments of the digestive tract
<http://training.seer.cancer.gov/images/anatomy/digestive/intestine.jpg>
------------------------------------
##
This NIH News Release is available online at:
<http://www.nih.gov/news/health/may2012/nci-21.htm>.
To subscribe (or unsubscribe) from NIH News Release mailings, go to
<http://service.govdelivery.com/service/subscribe.html?code=USNIH_1>.
If you subscribed via the NIH Listserv, go to <https://list.nih.gov/cgi-bin/wa.exe?A0=nihpress>.
{kind=link}
